Executive Summary
- On March 15, 2025, President Trump signed a continuing resolution, which included an extension of Medicare telehealth flexibilities through the end of September.
- Medicare telehealth coverage presents a myriad of benefits and drawbacks – with some studies suggesting greater access to care, potential cost-savings, and high quality of care coming at the expense of a widening healthcare cap, risk of improper payments, and certain care delivery limitations.
- Assessing the pros and cons of Medicare telehealth coverage will continue to drive discourse about the viability of its permanent policy adoption and its influence on health care outcomes.
Introduction
On March 15, 2025, President Trump signed a continuing resolution (CR) passed by Congress, which extends Medicare telehealth flexibilities through the end of September. These flexibilities –originally introduced via regulatory modifications and waivers in the wake of the COVID-19 Public Health Emergency (PHE) – allow all Medicare beneficiaries the option to access a wide array of telehealth services with reimbursements at parity with in-person visits.
Telehealth, which leverages the use of telecommunication and electronic information technologies to support long-distance healthcare, has seen significant growth since eligibility and payment flexibilities were enacted in 2020. While the expansion of telehealth coverage was crucial to maintaining a robust healthcare system during the PHE, its long-term viability remains a point of contention. This analysis provides a brief overview of the main pros and cons of Medicare telehealth coverage, as the future of telehealth policy is discussed.
Background
Telehealth Utilization Prior to the COVID-19 PHE
Prior to the COVID-19 PHE in early 2020, telehealth was a relatively small component of the American health care system in terms of patient utilization. In the year leading up to the pandemic, telehealth rounded to less than 1 percent of outpatient visits for large employer insurance enrollees, despite 82 percent of plans offering coverage and 53 percent of those plans offering cost-sharing incentives. Nonetheless, telehealth adoption by health care providers had been steadily increasing before 2020, with 76 percent of hospital systems offering at least one form of telemedicine service in 2018. Radiology, psychiatry, and cardiology represented the most utilized telehealth treatments – however, their “absolute integration” was fraught will problems surrounding reimbursement amounts and restrictions on technology.
For Medicare fee-for-service (FFS), telehealth coverage was restricted to a small portion of eligible beneficiaries – primarily for those in rural areas with scarce access to comprehensive healthcare providers. The Centers for Medicare and Medicaid Services (CMS) placed other strict regulations on telehealth coverage including provider eligibility requirements, technology specifications, and in-person evaluation prerequisites before telehealth services could be reimbursed. For those and other reasons, less than one percent of total visits by Medicare enrollees were conducted via telehealth in 2019; and in the first quarter of 2020, less than 7 percent of eligible enrollees used telehealth services at least once.
For Medicare Advantage (MA) enrollees, telehealth coverage was more extensive than traditional Medicare FFS, though utilization data remains limited in scope. By law, MA plans are required to cover all FFS benefits, including telehealth, with plans offering additional flexibilities depending on their payment model. Despite cost-sharing incentives for eligible enrollees provided by some plans, telehealth utilization among MA beneficiaries mirrored that of Medicare FFS and large employer-sponsored insurance plans. According to one study, the number of telehealth visits for eligible MA beneficiaries in 2019 was less than one percent of visits that would occur in the following year.
Telehealth Expansion After COVID-19 PHE
In late January 2020, the Department of Health and Human Services (HHS) declared a national emergency concerning the COVID-19 outbreak. In response, federal and state lawmakers explored alternative means of maintaining essential functions in healthcare. With limited time to react, expanding telehealth coverage quickly became a key strategy to meet rising healthcare service demand and to mitigate coronavirus transmission.
On March 6, 2020, President Donald Trump signed the Coronavirus Preparedness and Response Supplemental Appropriations Act, granting HHS and CMS the authority to allow broad flexibilities for telehealth coverage. In short, the bill clarified the HHS Secretary’s authority under section 1135(b) of the Social Security Act, allowing the department to temporarily waive Medicare telehealth requirements regarding provider participation, technology, physician licensing, and payments. Commonly referred to as 1135 waivers, the updated policies promoted a swift expansion of telehealth during the PHE.
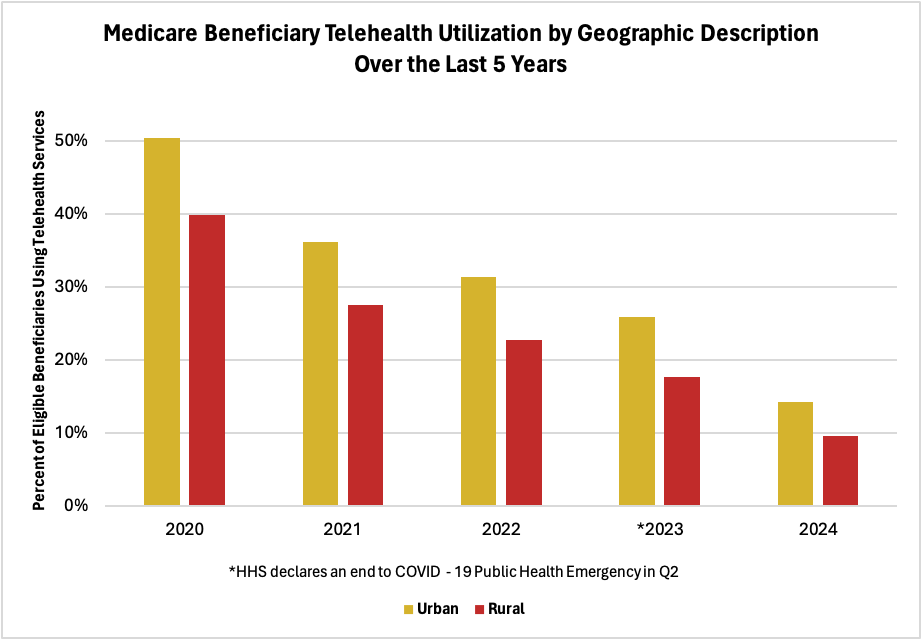
Following the passage of the Coronavirus Preparedness and Response Supplemental Appropriations Act, the issuance of section 1135 waivers, and the enactment of other supplemental COVID-19 relief legislation, telehealth utilization surged. By the second fiscal quarter of 2020, 47 percent of Medicare beneficiaries had used a telehealth service – which marked a near 600 percent increase from the previous quarter. Beginning in the end of 2020 and over the next three years, telehealth visits for Medicare beneficiaries gradually declined until plateauing at around 13 percent by the end of 2023 – months after HHS declared the PHE’s end.
Telehealth utilization among Medicare Advantage beneficiaries followed a similar trajectory to that of Medicare FFS, though some evidence suggests that adoption rose more rapidly and reached higher levels in MA. One study found that from mid-March to late April 2020, the share of telehealth visits among MA beneficiaries significantly exceeded that of FFS (see chart below). This trend was particularly notable among low-income and disabled individuals, who were nearly 20 percent and 7 percent more likely, respectively, to use telehealth services compared to their FFS counterparts. By the second fiscal quarter of 2020, telehealth utilization declined at a comparable rate in both programs, with approximately 1 in 4 beneficiaries using telehealth services by the Fall of that year.

Source: JAMA Network
Source: Medicare Telehealth Trends – Data.gov
Current Trends in Telehealth Utilization
Although telehealth utilization has declined since the onset of the PHE (see chart above), telehealth services remain an integral part of the U.S healthcare system. The Consolidated Appropriations Act (2021) and the Telehealth Modernization Act (2024) made certain telehealth flexibilities permanent; most notably for behavioral telehealth, which proved to be a viable alternative to traditional in-person care during the PHE. Today, approximately 1 in 10 Medicare FFS beneficiaries continue to use telehealth services – which is notably higher than pre-pandemic levels.
The Pros and Cons of Telehealth Coverage
The ongoing bipartisan support for extending telehealth flexibilities, as evident in the March 15 CR, suggests that lawmakers may look to make additional telehealth flexibilities permanent. Before committing to lasting provisions, Congress may find merit in evaluating the viability of telehealth coverage across a myriad of services – considering the fiscal impact on stakeholders, as well as its effect on healthcare outcomes.
The limited research on telehealth’s long-term effects lacks clear consensus. Some studies suggest telehealth enhances accessibility, cost savings, and patient and provider satisfaction; while others contend that telehealth contributes to poorer quality of care, an increase in the healthcare gap, and the potential for waste, fraud, and abuse.
Pros
1.) Accessibility
One of the most significant benefits of telehealth – and a core tenet of its rapid adoption during the PHE – is improved accessibility for patients and providers. In healthcare, accessibility refers to the ease, convenience, and reliability of care delivery. Proponents of telehealth argue that it reduces geographic, temporal, and practical barriers – which ensure that more individuals, particularly those in underserved areas, receive timely medical care.
Telehealth is especially critical for older adults and individuals with disabilities, who typically require more frequent healthcare services but may lack the ability to travel to appointments on their own volition. By offering remote telehealth services – including consultations, continuous monitoring, and speedy diagnoses – telehealth could have the potential to improve healthcare outcomes of vulnerable populations.
2.) Potential Cost-savings
The cost-saving potential of telehealth coverage remains a subject of debate among lawmakers and researchers. In theory, telehealth’s lower facility costs compared to in-person care could lead to a reduction in reimbursements for CMS and private insurance programs. A recent study, pending peer-review, found that 30-day Medicare spending for telehealth visits was 32 percent lower than in-person delivery of the same service. The study also noted that patient utilization rates remained consistent for both types of delivery. If these findings hold true, a permanent expansion of telehealth coverage could result in significant taxpayer savings in the future.
3.) Quality of care
Assessing telehealth’s impact on quality of care is challenging, as it involves monitoring many moving variables that are difficult to observe – but recent research suggests comparable outcomes to in-person delivery for many common treatments. An HHS policy review found that telehealth services maintained similar quality outcomes for patients with hypertension and type 2 diabetes. Moreover, in a separate study from 2022, it was determined that patients with the same chronic illnesses had fewer follow-up visits compared to patients receiving in-person care. Finally, a report from Harvard Medical School concluded that expanded telehealth coverage improved quality of care with only marginal increases to per-capita Medicare spending.
Cons
1.) Technology barriers & the healthcare gap
A major drawback of telehealth is its innate requirement for modern technology and broadband internet access, which disproportionately affects vulnerable populations. Individuals with disabilities and those in underserved communities tend to have limited internet connectivity, digital literacy, and sufficient hardware for comprehensive telehealth services – alluding to barriers beyond the purview of Medicare policy. Without targeted strategies to alleviate this divide in opportunity, full Medicare telehealth coverage risks widening the healthcare gap.
2.) Improper payments
Perhaps the biggest political hurdle in allowing permanent telehealth coverage is addressing the risk of waste, fraud, and abuse inherent to telehealth Medicare billing. In 2022, the HHS Office of Inspector General identified that 1 in 7 Medicare providers demonstrated “concerning billing” and posed a “high risk” of improper payments. The Government Accountability Office also raised concerns about the potential for improper payments in Medicare telehealth billing – recommending that lawmakers assess the quality of telehealth billing before flexibilities are made permanent.
3.) Health Care Delivery Limitations
Not all telehealth services serve as 1:1 substitute for in-person visits. Telehealth encompasses both clinical and nonclinical treatments, meaning some services do not involve direct patient care. Even telemedicine, which refers to remotely delivered clinical care, has limitations in treatment accuracy and feasibility. The inability to perform comprehensive physical examinations poses a significant challenge, as certain conditions cannot effectively be diagnosed without or treated without in-person evaluations. Moreover, the relationship between patients and providers is a critical aspect of health care delivery that remote visits can hinder. Many patients receiving specialty care prefer in-person visits due to the emotional connection and physical presence not fully present in telehealth services.
Conclusion
With Medicare telehealth flexibilities extended through the end of September 2025, health care stakeholders will have limited time to determine if permanent flexibilities are viable policy. Proponents point to research that has demonstrated telehealth services improving accessibility, potential cost-savings, and having comparable quality of care with in-person services. Detractors call attention to the risk of widening the healthcare gap, limitations in health care delivery, and hazards of waste, fraud, and abuse in Medicare telehealth billing. Further evaluation of these points will be necessary before a final decision can be made later this year.

You must be logged in to post a comment.